

Introduction
Midostaurin is the only approved FLT3 inhibitor for combination with intensive induction and consolidation chemotherapy in newly diagnosed patients with FLT3 mutant AML. The FLT3 inhibitor, sorafenib, was investigated in the randomized SORAML trial (Röllig, Lancet Onc 2015), in combination with intensive chemotherapy (IC) for newly diagnosed adults with AML <60 years. A sub-group analysis of 46 patients with FLT3-ITD, indicated a trend for improved overall survival (OS) in the sorafenib (SOR) arm compared to placebo (PBO).
Methods
The Australasian Leukaemia and Lymphoma Group (ALLG) conducted a randomized phase 2 study [ACTRN12611001112954] in 99 adults aged 18-65 years with newly diagnosed FLT3-ITD positive (allelic ratio (AR) ≥0.05) AML to determine whether addition of SOR to IC would improve event-free survival (EFS). The study was powered to identify a 25% increase in 2-year EFS with SOR. Patients 18-55 yrs received induction with IDAC-3 (idarubicin [IDA] 12 mg/m2 D1-3 and ara-C 1.5 g/m2 BD D1,3,5,7); patients 56-65 received 7+3 (IDA 12 mg/m2 D1-3 and ara-C 100 mg/m2 D1-7 IVI). Patients were randomized 2:1 to SOR or PBO 400 mg BD on days 4-10 of induction and each consolidation cycle. Due to the pharmacokinetic interaction between SOR and azoles, antifungal prophylaxis during induction was with AmBisome 5 mg/kg IV twice weekly. For consolidation, patients 18-55 yrs received 2 cycles of IcE (IDA 9 mg/m2 D1-2, ara-C 100 mg/m2 D1-5 IVI and etoposide 75 mg/m2 D1-5), those 56-65 yrs received 2 cycles of IDAC-2 (IDA 12 mg/m2 D1-2 and ara-C 1g/m2 BD D1,3,5). Maintenance was with SOR/PBO 400 mg bd days 1-28 for 12 cycles. Allogeneic HCT (allo-HCT) was at investigator discretion. SOR/PBO was not continued post allo-HCT. The primary endpoint was EFS without censoring for allo-HCT with events defined as failure to achieve complete remission (CR) or CR with incomplete hematologic recovery (CRi), relapse or death. Pre-specified secondary endpoints included overall response rate (ORR) defined as CR and CRi, tolerability, EFS according to FLT3-ITD AR < or ≥ 0.7 and impact of randomization on allograft outcome.
Results
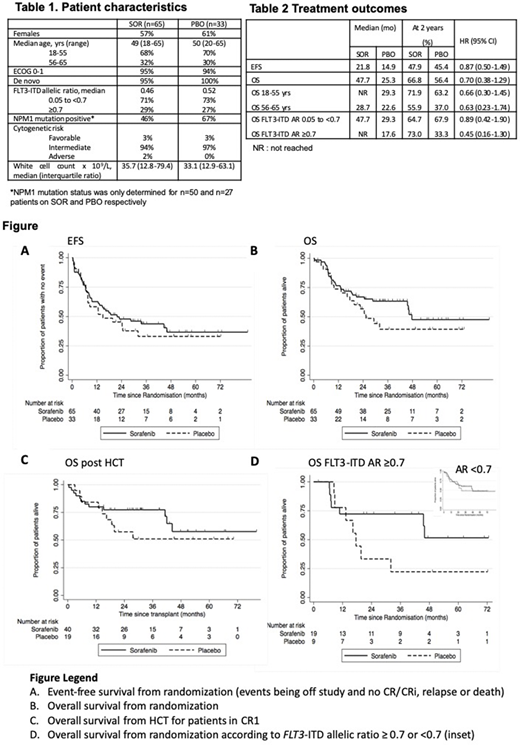
Between Jan 2013-May 2018, 18 centers randomized 99 patients to induction with either SOR (n=65) or PBO (n=33); one patient later found to be FLT3-ITD negative was excluded. Patient characteristics are shown in Table 1. Treatment arms were balanced apart from fewer patients in the SOR arm with NPM1 mutant AML. Deliverability of therapy was comparable, with commencement of consolidation in 78% and 79% and maintenance therapy in 32% and 27% in the SOR and PBO arms, respectively. The overall response rate (ORR) was high in both arms; 91% in the SOR (CR 80%, CRi 11%) and 94% in the PBO (CR 70%, CRi 24%) arm. In the SOR arm, 5% achieved partial remission, went off study and were deemed treatment failures. With a median overall follow-up of 25 mo, there was no significant difference in EFS (HR 0.87 95% CI 0.50-1.49; P=0.61)(Fig A) or OS (HR 0.70 95% CI 0.38-1.29; P=0.26)(Fig. B), nor in a sensitivity analysis with censoring at HCT. 2 yr EFS was 47.9% (SOR) vs 45.4% (PBO) and 2-year OS 66.8% (SOR) vs 56.4% (PBO). Hematopoietic cell transplant (HCT) in CR1 was performed in 62% and 58% in the SOR and PBO arms, respectively. For patients in CR1, 2 yr OS post-HCT was 78.5% (SOR) vs 54.2% (PBO)(Fig C). Suggestive of an on-target effect against FLT3-ITD, the impact of SOR on OS appeared greater for patients with higher FLT3-ITD AR ≥0.7 (Fig. D) (Table 2). Only one early death (within 30 days) was recorded in each treatment arm. The frequency of grade 3-4 adverse events (AEs) were similar between the two arms, apart from palmar-plantar rash, reported as drug-related in 15.4% and 6.1% pts in the SOR and PBO arms, respectively. Correlative studies will be reported in a companion abstract.
Conclusions
SOR did not improve EFS when combined with intensive chemotherapy in adults with newly diagnosed FLT3-ITD AML. Although not powered for significance, SOR showed a trend for improved OS among patients with higher FLT3-ITD AR or receiving HCT in CR1. Further exploration of more potent FLT3 inhibitors in the pre- and post-allograft setting are warranted for patients with newly diagnosed FLT3 mutant AML.
Acknowledgements: The ALLG AMLM16 trial was funded through an Australian Government NHMRC grant and a research grant from the Leukaemia Foundation of Australia. Bayer supplied sorafenib and Gilead AmBisome.
Wei:Roche: Honoraria; Servier: Consultancy, Honoraria, Research Funding; Novartis: Honoraria, Research Funding, Speakers Bureau; Amgen: Honoraria, Research Funding; Abbvie: Honoraria, Research Funding, Speakers Bureau; Pfizer: Honoraria; Bristol Myers Squibb: Honoraria, Research Funding, Speakers Bureau; Walter and Eliza Hall Institute of Medical Research: Patents & Royalties: AW is eligible for royalty payments related to venetoclax; Astra Zeneca: Honoraria, Research Funding; Janssen: Honoraria; Macrogenics: Honoraria. Enjeti:Novartis: Membership on an entity's Board of Directors or advisory committees; Alexion: Speakers Bureau; Bayer: Speakers Bureau; Sanofi: Speakers Bureau; AbbVie: Membership on an entity's Board of Directors or advisory committees; Astellas: Membership on an entity's Board of Directors or advisory committees. D'Rozario:Abbvie: Membership on an entity's Board of Directors or advisory committees; BMS/ Celgene: Membership on an entity's Board of Directors or advisory committees. Marlton:Celgene: Membership on an entity's Board of Directors or advisory committees; Janssen: Membership on an entity's Board of Directors or advisory committees; Astellas: Membership on an entity's Board of Directors or advisory committees; AbbVie: Membership on an entity's Board of Directors or advisory committees; F. Hoffmann-La Roche Ltd: Membership on an entity's Board of Directors or advisory committees; Astra-Zeneca: Membership on an entity's Board of Directors or advisory committees; Novartis: Membership on an entity's Board of Directors or advisory committees. Verner:Janssen Cilag Pty Ltd.: Research Funding. Hahn:Roche: Honoraria; Astra Zeneca: Honoraria. Hiwase:Novartis Australia: Research Funding. Anstee:Walter and Eliza Hall Institute: Patents & Royalties: milestone and royalty payments related to venetoclax.. Levis:FujiFilm: Honoraria, Research Funding; Amgen: Honoraria; Daiichi-Sankyo: Honoraria; Menarini: Honoraria; Astellas: Honoraria, Research Funding. Bajel:Abbvie: Honoraria; Astellas: Honoraria; Pfizer: Honoraria; Amgen: Honoraria, Speakers Bureau; Novartis: Honoraria. Roberts:Genentech: Patents & Royalties: for venetoclax to one of my employers (Walter & Eliza Hall Institute); I receive a share of these royalties; Janssen: Research Funding; Servier: Research Funding; AbbVie: Research Funding.
Sorafenib for FLT3-ITD AML

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal